If you are an owner of a pediatric office located within the United States, chances are you answered no to this question – and may not even be aware of it.
Pediatric billing has its own unique characteristics as compared to other specialties. As an example, there are CPT codes based on ages, complex rules attached to vaccine administration, modifiers must be used depending on the type of service provided, there are nuances associated with Medicaid, CHIP, etc, as well as constantly changing payer-specific policies; all contribute to the very slim profit margin available to you. Studies show that the average rate of denied claims in all specialties is approximately 20% and that approximately 60% of those denied claims were not resubmitted. For a busy pediatrician who sees dozens of patients a day, this can translate into hundreds of thousands of dollars leaking out of their revenue cycle over time.
A pediatric billing audit is what stops these leaks from happening. A pediatric billing audit is the most impactful diagnostic tool you can use to identify hidden revenue drains within your practice, fix systems errors that may exist, and create a billing process that works as hard as the rest of your business does.
At The Medicators, we have helped pediatric offices across America recover huge amounts of lost revenue through structured specialty-specific billing audits. This guide will give you a comprehensive overview of what an audit uncovers, where most practices lose money, and how to fix these issues permanently.
What Is a Pediatric Billing Audit? – The Medicators’ Expert Breakdown
The pediatric billing audit is a thorough look at your practice’s billing and payment history for 90-180 days to discover discrepancies between what you provided the patient and what was collected from you.
Pediatric billing is different than general fights so a pediatric audit reviews many things that a general audit would not cover; i.e.; Coding for well visit (based on age), Vaccine product (used) + Admin codes (used), Services billed in dual (Modifier 25 used), Bundling by payors for developmental and behavioral screening (also by payor), and State Mod & CHIP rules (very specific to that state).
Practices doing an audit for the first time typically discover 3-5 large leaks in where they have lost revenue that they were not aware of. This is a lot of money, and these audits have been known to change practices.
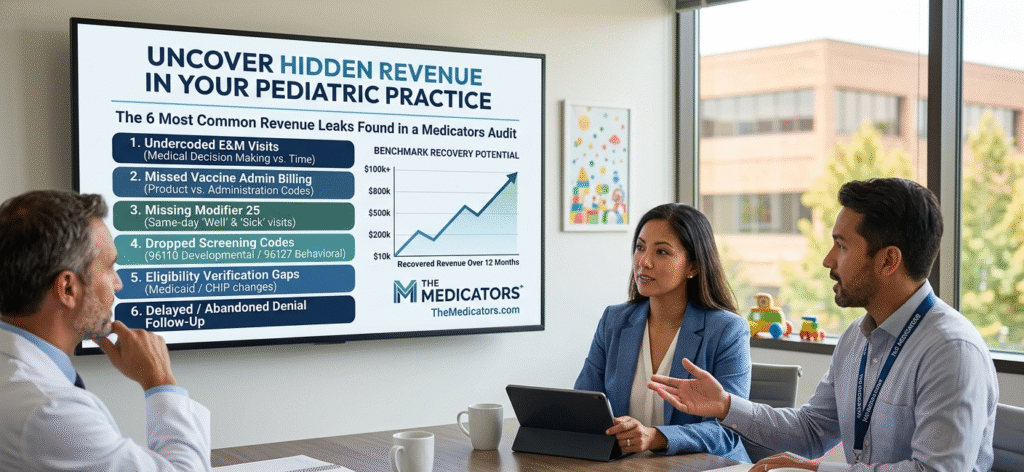
The 6 Most Common Revenue Leaks The Medicators’ Pediatric Billing Audit Reveals
1. Undercoded Evaluation & Management (E&M) Visits
In the realm of pediatric billing, coding complexity (the way the billing company codes a bill for a service) is the leading revenue leak. In other words, coding complexity is responsible for more than half of all claims denied in pediatric practices.
When a physician meets with a complex patient for 25 minutes or 30 minutes and submits a Level 2 visit (99212 or 99202), they are leaving significant amounts of reimbursement on the table. Starting in 2026, E&M coding will be based on either Medical Decision Making (MDM) or total time, meaning that providers who are diligent in their documentation will be able to code their office visits (both new and established) at levels higher than they typically would through habit or apprehension.
By creating a billing audit that compares the complexity of the documentation against the CPT codes that were billed, you will quickly discover coding patterns by your providers consistently coding below what the documentation states.
Your solution is to train your providers on how to utilize the current MDM table as found in the AMA fee schedule. For example; the difference between an established patient visit at Level IV versus Level III is $40-70 per visit. If you have 20 ways to service patients per day, this is a $200,000 loss in revenue for the year based on this under-coding.
2. Missed or Incorrect Vaccine Billing
The financial foundation of nearly all pediatric practices is built upon vaccinations as well as billing for vaccines can also be one of pediatrician’s most common mistaken billing practices.
Each vaccination visit is made up of 2 separate billable parts: (1) the product code for the vaccine (e.g., DTaP has the product code 90700) and (2) the vaccine’s administration code (90460 for the first service with counseling and 90461 for each subsequent service). Omitting to use the administration code and/or using 90471 or 90474 when counseling was documented results in underpayment or a denial.
During the audit each Medicator verifies the accuracy of the vaccine inventory records compared to the vaccine claims submitted for reimbursement. If the number of doses administered does not match the number billed to insurance, there is revenue that has been lost; For example, in a practice that gives over 50 doses of vaccine per day, even a 10% billing error translates into thousands of dollars of lost revenue per month.
In addition to claiming revenue losses, inaccurate vaccine inventory records also present compliance risks due to improper accounting methods between private and VFC mixed inventory. In order to correctly account for the amount of vaccine billed against what is VFC funded, the audit distinguishes those that the billing department is responsible for and those that are VFC funded (and must therefore not bill). While most billing departments handle in-house VFC invoices correctly, it is not true across the board for each doctor’s office across the country.
3. Missing Modifier 25 on Dual-Service Encounters
Billing errors involving pediatric billing is one of the most frequently cited and costly mistakes made in pediatric health care. The two separately billable services are billed when a child receives a well-child exam in addition to receiving treatment rendered on the same date for an acute condition (i.e., ear infection, cough, etc.).
For this encounter, there are 2 separately billable services that will need to be billed: the Preventive Visit (well-child exam) and the Sick Visit (E&M visit for treatment).
The Preventive Visit for children aged 1–4 can be billed using the E&M code (99392); whereas the Sick Visit for treatment of an acute problem can be billed using the applicable E&M code (e.g. 99213).
In order to receive payment for both Preventive and Sick Visits on the same date of service, Modifier 25 must be applied to the Sick Visit E&M code in order for the payer to recognize that a separate and distinct service was provided in addition to the service provided during the Preventive Visit. If Modifier 25 is not used on the Sick Visit E&M code, then, the payer will “bundle” the 2 services and only pay for the Preventive Visit.
Billing audits assess claims billed for dual-service encounters where claims are audited to determine how often Modifier 25 was either missing, incorrectly applied, or applied without adequate supporting documentation. In situations where the chart does not clearly differentiate the Preventive and Sick Visits from each other, a claim, with or without the application of Modifier 25, can be denied when audited, regardless of whether or not the claim was completed correctly.
4. Dropped Developmental and Behavioral Screening Codes
In the realm of pediatric medicine, developmental and behavioral screenings feature highly on the list of services being billed poorly when they should actually be regularly billed.
For example, both the use of 96110 – Developmental Screening (e.g., Ages & Stages Questionnaire) and 96127 – Behavioral/Emotional Assessment (e.g., Vanderbilt ADHD Scale, M-CHAT) are examples of commonly used codes that are typically billed together with other clinical services but not necessarily billed separately for some payers.
A billing audit of the individuals you are serving in your practice will provide you with information about the types of payers in your practice and if they allow for separate billing of these two services. Many practices feel they cannot bill for these services separately and give up on trying, resulting in a constant loss of revenue each day.
5. Eligibility Verification Gaps Causing Downstream Denials
A billing audit considers more than just the submitted and billed codes; it also takes into account factors before any claims were submitted or billed. One of the easiest ways to prevent denials for a pediatric claim is to ensure accurate and current insurance information.
Due to the following factors, children with Medicaid or CHIP have significantly higher rates of changes to their insurance than adults: children “age out” of their parents’ insurance, parents change jobs, income-based eligibility for Medicaid can change at any time as well as there can be dual insurance for both parents.
If your team is not verifying eligibility at every single visit, including established patients, you’re going to submit claims into a void. A billing audit will quantify the total number of denials that can be traced back to an issue with that patient’s eligibility, which is almost always greater than practices expect.
6. Delayed or Abandoned Denial Follow-Up
In addition, an audit will also uncover what happens to all of your claims related to pediatric denial management. Many practices find that their process for managing denied claims is either inconsistent at best or doesn’t exist at worst. They become stagnant; they are “in limbo” awaiting resolution. There are times when appeals for denied claims expire; therefore, revenue that could potentially be regained is not recouped.
Research has found that over 50% of all claims appealed are ultimately paid once followed-up by someone. By conducting a billing audit, you will find your current denial rate (high-performing practices target below 5%), your appeal rate, your recovery rate, and what specific codes for denied claims appear most often which enables you to put systemic solutions in place.
The Medicators operate with a zero write-off culture; therefore, every denied claim should be reviewed, responded to, or appealed to collect payment prior to being written off.
Key Billing Metrics The Medicators Tracks in Every Pediatric Audit
An effective pediatrics billing assessment is not only about identifying issues; it also provides you with a set of performance metrics to help you determine where you stand.The above are the benchmark metrics that are most important for you to consider:
- Days in A/R – Under 30 days
- A/R Over 90 Days – Under 15% of the total amount of A/R
- Clean Claim Rate – 95%-99%
- Denial Rate – Under 5%
- Net Collection Rate – 95%-99%
- Patient Collection Rate – 90%+
If your practice is not meeting one or more of these benchmarks, the analysis will indicate why and which areas you should concentrate on for your first efforts to address the issues.
Internal vs. External Pediatric Billing Audit: Which Do You Need?
Many practices will attempt to conduct internal audits of their own billing department; while a review of any type is better than nothing, there are major limitations to doing an internal audit. First and foremost, the same team responsible for making the errors is now the same team reviewing how those errors were made. Their objectivity has been compromised. Secondly, rarely do internal staff have the time or pediatric-specific knowledge required to perform an exhaustive review of multi-payer or multi-code billing.
A pediatric-specific external audit, performed by a company of specialists such as The Medicators, provides a different level of scrutiny. In this case, we bring pediatric-specific coding knowledge to your practice and will perform a comparison of your practice’s performance to national benchmarks. We will also review each of your payer contracts for patterns of underpayment as well as identify compliance issues that the internal teams will frequently overlook.
In fact, for the majority of pediatric practices, an external audit will pay for itself multiple times over in recovered revenue during the first 90 days following completion of the audit.
How The Medicators Conducts a Pediatric Billing Audit — Step by Step
The Pediatric Billing Audit conducted by The Medicators follows a clearly defined structure that was designed with an emphasis on data. Each aspect of the audit is tailored specifically to match your pediatric practice’s unique payer mix, patient volume and EHR system and includes five major steps outlined below.
Step 1
Claims Data Analysis: A complete collection of 90 – 180 days of claims data is gathered from your existing patient accounts then processed through our pediatric billing audit framework. We will identify any undercoded visits, any missing modifiers, any dropped vaccine codes and any unbilled screenings.
Step 2
Denial Pattern Review: We will categorize all denials using the unique code that the insurance company has assigned as the reason for denying the claim. This process allows us to identify recurring denial patterns, as well as to estimate the total amount of lost recoverable revenue currently sitting in your denial queue as a result of these repeated denial patterns.
Step 3
Payer Contract Review: We compare the reimbursement you receive from payers against what you are contracted to be reimbursed. Identifying and quantifying systematic underpayment is one of the largest potential categories of revenue loss that most practices covet; however, identification of systematic underpayment generally requires that a practice engage the services of an external auditor.
Step 4
Documentation Support Review: We will evaluate whether your clinical documentation supports the codes billed by the provider performing the visit. If medical record documentation and codes billed are at different levels, we will provide our client with a report-thus identifying whether the nature of documenting at a higher level constitutes overcoding (a compliance risk) and whether documenting at a lower level constitutes undercoding (a revenue loss).
Step 5
Actionable Audit Report and Implementation Support: You will receive an in-depth audit report containing specific findings, estimated dollar amount that can be recovered based on success of each claim and an action plan detailing the steps necessary to implement corrective action. Instead of just handing you your report and leaving, we will assist you in implementing the required changes.
The ROI of a Pediatric Billing Audit: Real Numbers
For a pediatric practice of around 60 patients, approximately 240 days/year, will have 14,400 total visits in one year.
Missed Modifier 25 Opportunities:
15 percent of the well child appointments could yield between $40,000 – $60,000 of unbilled dual-service revenue on the average $14,400 in revenue.
Under-Coding of E&M Visits by One Level on Average:
Usually around $100,000 in lost revenue potential.
Number of Vaccine Coding Errors:
10% of total visits could lead to $20,000 – $40,000 in lost revenue.
Collection Denial Rates:
10%, as opposed to the benchmark for denial, which is 5% = 10’s of thousands $’s in disastrous expected losses.
A thorough pediatric billing audit can help identify and recover a portion of the revenue that you have already earned as a result of your practice.
Start Recovering What You’ve Already Earned – Partner with The Medicators
Your pediatric business is working too much and your staff is genuinely concerned about losing money because of billing problems. No matter if your issues are chronic undercoding, high denial rates, inconsistent vaccine billing, or not reviewing your fee schedule in years, conducting a structured audit of your billing is the most important and first step to addressing anything happening with your revenue.
The Medicators has over 20 years of experience in the medical billing field (and well as being pediatric coding certified) with a 99% clean claim rate in our audits. When we perform billing audits for you, our audits are not merely a review of your practice’s billing, but rather a pathway to improving your practice’s revenue.
The Medicators – Taking You Forward.
Serving individual practices, group practices, and hospitals nationwide.
204 F St, Unit B2, Davis, CA 95616 | 24117 W. 103rd Street, Suite L, Naperville, IL 60564
+1 (888) 277-1460 | info@themedicators.com
Ready to find out what your practice is missing?
Request Your Free Pediatric Billing Audit →
Call us at +1 (888) 277-1460
email info@themedicators.com
Our team is available 24/7.
Frequently Asked Questions (FAQs) — Pediatric Billing Audits
Q1. What is a pediatric billing audit and why do I need one?
A pediatric billing audit is a claim, coding, and payment comparison to locate any errors, missed revenue, and compliance issues. It will help identify any lost revenue that might occur due to specific issues associated with pediatric billing.
Q2. How often should a pediatric practice conduct a billing audit?
A practice should perform at least one audit annually. Practices with high patient volumes or high denial rates may benefit from performing an audit quarterly and conducting ongoing monthly monitoring as well.
Q3. What is the most common billing mistake in pediatrics?
The most common cause of undercoding occurs when E&M visits are coded lower than the level dictated by the documentation and results in the loss of a large amount of revenue.
Q4. What is Modifier 25 and why does it matter?
Modifier 25 is used when an E&M service is rendered on the same day as another procedure to provide reimbursement for both types of services properly.
Q5. How is The Medicators’ audit different from in-house review?
The Medicators can assess and verify your patterns, payments, missed revenue and more, often identifying items that may not have identified by a group working internally.
Q6. Can a billing audit help Medicaid and CHIP issues?
For example, eligibility errors could be identified; state-specific coding concerns could be identified, and the common errors within Medicaid/CHIP billings for underpayments.
Q7. What codes are most commonly missed?
Additional frequently missed billing codes include vaccine administration (90460/90461), screening (96110, 96127) and add-on (99415) or preventive service (99173) codes.
Q8. How long does an audit take?
For small practices, it typically takes two to three weeks for completion of the billing audit, while for larger practices, this can take four to six weeks, depending on the complexity of the data provided.
Q9. What do I receive after the audit?
The bill audit consists of a detailed report, with information regarding errors made on claims, estimated revenue lost due to errors made, and an analysis of claim denial trends, as well as a prioritized plan to correct the errors going forward.
Q10. How much revenue can be recovered?
Many practices that successfully correct both undercoding and underbilling opportunities can recover tens to hundreds of thousands of dollars per year.
Q11. Is it the same as a compliance audit?
A billing audit is based on issues related to revenue capture, while a compliance audit focuses more on the accuracy of coding and the risk associated with compliance. Typically, billing and compliance audits are conducted together.
Q12. How do I get started?
You can request an audit through The Medicators or call +1 (888) 277-1460 to begin the process.