You turned in a claim without errors. You used the right coding, the treatment matched the diagnosis, and you verified the modifiers. Even though everything was properly coded according to the patient’s file, the claim was still denied. The vast majority of your peers are experiencing this same demoralizing lack of payment for their work because it is not due to inaccurate coding.
A vast majority of the billing departments within health systems are working very hard to have their diagnoses (ICD-10 matches) and procedure codes (CPT) all matched until they are perfect. After a claim was filed and assigned with proper ICD/CPT, it will still be denied due to reasons that are totally unrelated to code matching. In a recent study done by Experian Health, 73% of respondents within the healthcare community experience increasing trends in claims denials; this has grown substantially from just 22% of responses since 2022.
Today, the average non-Medicare-related claims denial rate usually deviates between 5-10%. Meanwhile, denial rates for the Medicare Advantage payer have increased to the 15%-20% range. This is clearly not due to (incorrect) coding; this is a systems issue; this systems issue begins with a clear understanding of where the source of “unrealized” denials exists.
Why “Accurate Coding” Is No Longer Enough
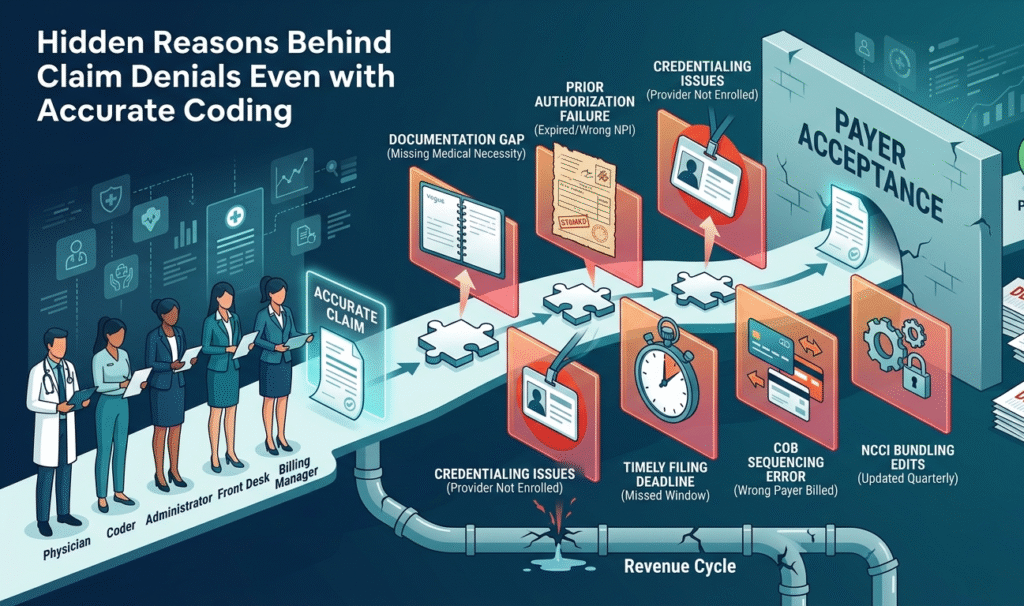
It is possible to code a claim perfectly according to coding rules and still have it denied. The problems causing this denial may come from upstream and downstream from the procedure code on the claim; they may be related to the quality of the documentation, the nature of the payer agreements in place as it relates to the provider’s credentials, or so-called “timeliness.”
Think about a claim as a puzzle. If you get all the codes right, it means you put together all the pieces correctly to form a finished puzzle. However, if you have to fix your boundaries (meaning prior authorization was not received, the provider was not credentialed by that particular payer, or the information was received one day past the filing date), your puzzle will never be finished.
The AAPC published a report in 2024 regarding the salaries of coders in the industry. In regard to coding, their findings indicate an average reduction in claim denials of 23 percent due to credentialed coders compared to those who aren’t credentialed. Progress has been made; however, there are still lots of denials, which coding expertise alone will not be able to close.
Your Notes Don’t Say What You Think They Say
Even when the coder has coded everything perfectly. The provider has documented his/her visit as he/she saw it, and the coder has coded it correctly. However, the clinical language between the doctor’s notes does not directly tie the diagnosis to prove a medical necessity to complete the procedure; therefore, the payer will not make an inference, and as a result, they will read your notes.
According to the CO-11 denial pattern, “initially appearing to be a coding error is often found to be a lack of documentation that cannot be resolved with a corrected code alone.” This is especially true in the case of templated notes. When your EHR populates standard language for each patient that has the same condition, the insurance company’s system cannot rationalize that the patient required this procedure on this date.
The solution is not the creation of a new code; instead, the development of a new documentation practice is what will resolve the issue.
Medical Necessity Failures Under LCD and NCD Criteria
This will be much more difficult than initially believed. Your claim may be denied even if your service is actually a medical necessity if the documentation does not satisfy the specific language required in the Local Coverage Determination (LCD) or National Coverage Determination (NCD) that governs your area.
NCDs are issued by CMS and are required to be followed by all states. LCDs are created by Medicare Administrative Contractors (MACs) and are therefore unique to each region of the country. Because of these differences between regions, a CPT code can be billed in Texas and receive payment, while the same CPT code billed in California may be denied for the same service under LCD rules.
For example, if you bill CPT 93000 (electrocardiogram) with an ICD-10 diagnosis code of Z00.00 (general check-up), and the LCD for that region does not cover routine electrocardiograms, your claim will be denied, even if the service meets all of the requirements for being covered as a medical necessity.
To prove medically necessary care, the ICD-10 code must appear on an approved LCD list. In many cases, there has been a 70% increase in the number of denials based on medical necessity since 2016; the recently released 2024 CMS Interoperability & Prior Authorization Final Rule (CMS-0057-F) adds additional requirements for payers that will increase standardization around the reason for every denial due to medical necessity, effective January/2026. As of 2023, the average administrative cost per individual denial claim is $57.23, with an increase from 2022’s average administrative cost of $43.84, and is projected to continue to rise.
Why Are Vague Physician Notes Still Causing Denials in 2025?
The answer is fairly straightforward: the copy and paste culture. Physicians who have limited time frequently reuse prior notes for patients, and the notes typically do not have the detail needed for payer reviews. For example, a note for “patient is diagnosed with lower back pain and has been referred to physical therapy” would not support the same level of claim as “patient has returned to me with lumbar radiculopathy and has had no improvement with conservative care over the last 6 weeks; physical therapy ordered per published LCD guidelines.”
While the difference in the above example is not a clinical difference, it is a linguistically based difference, and the linguistic difference results in a loss of real dollars to the practice.
When You Got Auth, But It Wasn’t the Right Auth
When a provider does not obtain an authorization for a service, one expects the provider to receive a denial, providing that the authorization was obtained; however, many billing managers find themselves confused when they submit a claim with a valid authorization and get denied. More times than anyone cares to admit, an authorization is used for an unrelated service and, thus, denied.
For instance, if an oncology provider has a valid authorization for chemotherapy, yet their claim bill includes separate hydration that also requires an authorization, the provider will receive a denial due to the separation of services. Similarly, if an authorization includes the incorrect rendering of NPIs/Tax IDs, the provider will also receive a denial for that reason as well.
Payers have been more and more specific about authorizations needed for specific services recently, which is a change from previous trends within the Medicare system. The OIG’s recent report on Medicare Advantage plans showed that 13% of prior auth denials met Medicare coverage but were denied due to the “authentication issue.”
Expired authorizations are common in busy practices. A practice may have an authorization for a service, but when the appointment is moved, there is usually nobody at the practice that checks the auth window again to confirm the new date remains within that auth window timeframe, if the authorization is within timeframe, service is provided, claim submitted, and when the claim receives a denial due to the auth expiration on the date of the service.
This is not a failure of the coder. It is a failure of the process. Authorization management needs its own tracking system. Not a sticky note, a mental note, or assuming anything.
Credentialing Problems That Look Like Coding Errors
Billing Before Credentialing Is Finalized
When a new provider joins a practice and sees patients prior to completing the credentialing process with a given payer, every claim submitted to that payer will be denied. Billing for services while the credentialing process is still pending may be considered to be misrepresenting the provider as eligible to provide those services. This is a compliance issue, not just a billing issue. Failure to properly credential the provider before submitting claims for payment may cause timely filing for those claims to be lost. The CO-185 denial code (“provider not eligible to perform service”) is the formal statement of this issue.
Taxonomy Codes and NPI Mismatches
A provider’s NPI is currently active, but the taxonomy code, which is the field that identifies the provider’s specialty, does not match what the payer has on record. This results in an automatic denial of the claim, which is often the case when a provider transitions between practice settings (for example, from an outpatient clinic to an inpatient hospital setting) or when a group practice restructures its billing arrangement.
The solution to this problem involves confirming current and consistent taxonomy codes with both the NPI registry and each payer’s internal records.
Why “On Time” Means Different Things to Different Payers
Every payer has their own timely filing window, and those windows can vary significantly. Some commercial plans require claims to be submitted within 90 days of the date of service, while others can accept claims up to 12 months after the date of service. In addition, while Medicare typically allows a 12-month filing period, many Medicare Advantage plans have stricter internal deadlines.
The CO-29 denial will be issued for late claim submission when a claim is received after a payer’s timely filing window. In addition to not being able to appeal CO-29 denials, claims that have otherwise been completed accurately are almost uniformly denied if they are refused because they miss the timely filing deadline, and there are only narrow exceptions to this rule – such as occasional system outages and/or specific CMS administrative rules that apply in the case of government entities.
This demonstrates how a real-world scenario drives this home. A physical therapist provides services on June 1, 2024, but due to staff turnover, the claim isn’t transmitted until June 10, 2025, which is just 9 days past Medicare’s 12-month window. Therefore, that claim is permanently denied, and that revenue is lost.
The Resubmission Trap
Many practices lose timely filing battles not just on the original claim, but also on the resubmission of corrected claims. A claim is denied in month 2. The practice works to correct the claim; by the time the corrected claim is submitted, the filing window has already expired for that claim. Therefore, practices must track the timely filing deadline based upon the original date of service, not the date that the claim was denied, for every resubmission.
Coordination of Benefits and Payer Sequencing Errors
Billing the Wrong Payer First
When a patient has dual coverage, it matters a great deal how you bill the insurers. You must bill the primary payer first; then only will a secondary payer be able to pay. If you bill the secondary payer first or bill both payers at the same time without first establishing what was covered under the primary payer, the claim will be denied for improper billing sequences.
Insurers change as patients do. A spouse may be terminated from their employer insurance; Medicare becomes the primary insurer once the patient retires, etc. These changes do not always manifest at the front desk. When they do not, the patient’s coordination of benefits on record will be incorrect.
How Incorrect COB Data Snowballs
A single obsolete insurance record leads to several denials in the following manner: an improper carrier for the initial claim gets denied, and a claim from the secondary carrier can’t be processed without the settlement from the primary carrier. When all this gets resolved, and the correct billing order is corrected, some will not be paid due to the expiration of the time limits for filing the claims with the insurance companies after the resolution of the initial problem. Claims will be denied due to these same reasons if the verification of the CO B is not checked on all patients at every appointment, not just on initial appointments. It should be considered a part of daily front desk work. However, on those busy mornings at a medical clinic with multiple patients, this process is likely to be missed on the fifth patient, as time is not available.
NCCI Bundling Edits and Payer-Specific Rules
When Correctly Coded Services Get Bundled Out
Each quarter, NCCI releases an edit of the CPT codes in their bundling edit of two CPT codes for billing purposes for each patient seen by the practice. The guidelines for billing both CPT codes on the same date of service for the same patient. As a general rule, in each state, if the provider bills both codes on the same date of service for the same patient, the lesser code will be denied due to bundling, as the lesser code will always be considered the component of the greater code from the same company per CMS (for those coding services correctly).
Billing teams frequently encounter issues because the NCCI edits are updated approximately once every three months. It is very common for one coding pair to have been paid as separate services in January and then become bundled in April. If your billing or claim scrubbing software hasn’t been updated with the new NCCI tables, you won’t find out it was bundled until the service is denied.
For example, if you bill a CPT code for an Unna boot application (29580) along with surgical debridement codes (11042–11047), on the same anatomical site, without the XS modifier, you will receive a denial based on the 2022 NCCI Chapter 4 update, even if you accurately coded both procedures and legitimately performed both of them.
Payer-Specific Bundling That Goes Beyond NCCI
Commercial payors also have their own proprietary bunding rules beyond the NCCI guidelines published by CMS (8/2022). Therefore, one service that Medicare pays as a separate service may be bundled with another service (by Blue Cross), depending on the contracts and agreements between payors. Most healthcare providers do not review their contracts in detail, so they do not see these inconsistencies.
This is where working with a revenue cycle team that tracks payer-specific edits (not just standard NCCI edits) pays for itself quickly.
Contract and Fee Schedule Misalignments
The CO-45 Denial: What “Charges Exceed Contracted Rate” Really Means
A CO-45 denial code indicates the provider billed at a level greater than that of the maximum allowed for the contracted service or procedure. The reason this can seem confusing is that sometimes providers will not know that their contracted rate has changed until they receive a CO-45 denial code.
Payer contracts will renew; fee schedules can be updated, and then Medicare publishes annual Physician Fee Schedule changes. If your charge master (the internal list of charges you are billing) hasn’t been updated along with these changes, you will continue to bill at rates that are greater than the payer is going to pay, not because you are committing fraud, but because both sets of numbers are no longer aligned due to administrative changes that have caused the codes to be out of sync with each other.
One small-to-medium-sized cardiology practice (the name of which shall remain anonymous) received numerous CO-45 denials on claims that utilized the echocardiogram CPT code 93306. Many of the root causes for the CO-45 denials were due to using incorrect modifiers and old fee schedules, resulting in claims being submitted with fees that were above what was on the payer’s fee schedule.
Out-of-Network Denials for In-Network Providers
A provider may be hospital credentialed in-network with a particular payer’s group level, but the NPI that this provider is submitting their bill under is not credentialed in-network to submit a claim as an individual. Therefore, the claim will proceed as an out-of-network claim. This creates an increased cost-sharing liability for the patient, resulting in patient complaints to provider management, but it may take the billing department months to determine the root cause of the complaints before they can fix the problem.
The solution involves conducting regular credentialing audits to ensure that all rendering providers are properly enrolled and included in the networks of all payers in their contracts.
Claim Submission Errors That Fly Under the Radar
Wrong Place of Service Code
The place of service (POS) code identifies the location where a service was provided. If the incorrect code is provided, then the payer may not process the claim properly, regardless of whether the CPT (current procedural terminology) and ICD-10 codes are accurate. Telehealth claims are especially prone to this issue since there are differences in how Medicare and commercial payers reimburse telehealth services based on the payers’ respective POS codes for virtual visits (i.e., POS 02 vs. POS 10 vs. POS 11).
As of January 1, 2026, the updated Medicare telehealth site-of-service code rules changed how certain virtual encounters would be billed. The practice of continuing to use the old billing template will adversely affect practices by causing denials of telehealth services that were performed between January and May 2026 because the corrected claims contained incorrect codes.
Duplicate Claim Flags
Duplicate claim flags (CO-18) are issued by the payer when they believe they have previously received a claim for the same service. Duplicate claims are often erroneously flagged when a corrected claim is submitted without an appropriate corrected claim frequency code, causing the payer to view the second submission of the corrected claim as a second submission of the original claim rather than a replacement of the original. The corrected claim will remain in the denial queue while the original claim remains unpaid, thereby causing the revenue cycle department of the practice to back up due to inaccurate submission methods.
A Systematic Approach to Finding Your Hidden Denial Causes
To effectively decrease denials, it is imperative to examine the patterns behind them and understand what portion of the revenue cycle is being affected by failures, as opposed to simply correcting claims more quickly after they are denied.
For instance, begin with the following steps to help identify your denial patterns:
- Categorize the root cause of your denials, and separate your coding-related denials from those related to administrative, credentialing, authorization, and payer contract as needed. Many practices are shocked when they discover that the majority of their total denial volume is due to factors other than coding errors.
- Create payer matrices with each payer’s timely filing requirements; build matrices that include filing windows, authorization needs, and specialty-specific billing requirements; and make sure to update this information at least every three months.
- Audit credentialing status for active providers at the end of every quarter by checking your active provider roster against each payer’s in-network provider list and proactively correcting any discrepancies you find.
- Re-validate COB (coordination of benefits) at the time patients check in for their visits to your facility; do not rely solely on COB validation at the time patients come in for new patient appointments or at year’s end.
- As part of your ongoing process improvement efforts, ensure that you keep updating your NCCI and LCD tables from your third-party clearinghouse or billing system; failure to do so will leave you with no clear understanding of the criteria related to bundling or medical necessity.
- Read your payer contract. Payer-specific bundling language, the authorization window for authorization, and the timely filed provisions that are different from standard CMS rules should all be checked in the payer contract.
The Medicators’ Perspective: Denials Are a Systems Problem
We’ve examined denial patterns in dozens of specialty groups and found that the vast majority of denial reasons have nothing to do with clinical errors, but rather with process errors that are not being fixed.
The good news is that procuring raw, accurate, and actionable data through processes can solve process errors. By ensuring visibility, using appropriate timeframes and roles within your organization, as well as understanding where your organization resides in the revenue cycle timeline, implementing a structured denial management program that relates the denial codes and tracking the actual root causes of those denials (documentation gaps, coder training needs, authorization tracking failures, credentialing gaps), will help build secure revenues over time.
Having accurate coding is only a prerequisite; what differentiates between practices with revenue denial rates of 3% and those with 15% is the system that surrounds the claims.
Conclusion: Stop Fixing Claims and Start Fixing the System
Good intentions do not protect you from a claim denial. A claim might not get paid due to reasons such as an expired authorization, a credentialing gap that was created several weeks ago, or a coverage determination by the payer that was not known to the billing department as being applicable to the specific patient and location of the service.
The organizations that are successful in managing their revenue cycle are not necessarily those with the highest quality coding staff; however, coding staff quality is important. These organizations have developed strong pre-claim workflows, including quarterly reviews of Local Coverage Determinations and National Coverage Determinations, as well as conducting routine credentialing audits and coordinated benefits verification before each patient encounter.
Through understanding the hidden reasons behind claim denials, you begin to protect your revenue proactively, rather than only after a claim has left your office.
FAQ: Hidden Reasons Behind Claim Denials
What is the most common hidden reason for claim denials despite accurate coding?
Documentation errors, specifically, clinical notes that fail to demonstrate the Payer’s medical necessity guidelines under either a Local Coverage Determination or a National Coverage Determination, and therefore cause the claim to be denied.
Can a claim be denied if prior authorization was obtained?
Yes, if the authorisation is for the correct service, date range, or supplier NPI, the claim will be denied as long as there is still an authorisation number stored.
What is the CO-29 denial code?
A claim filed outside the timeliness period will be considered a CO-29, and no matter what code is billed will be denied and non-appealable.
How do NCCI bundling edits cause unexpected denials?
NCCI edits are updated on a quarterly basis, and therefore, pairings that were billed separately and paid in one quarter may be bundled in the next quarter, resulting in denials of any previous claim.
What is the CO-185 denial code?
CO-185 indicates that the rendering provider was not eligible to perform the service being billed. This happens when the provider bills the service before being credentialed with the payer.
Why does dual insurance coverage cause claim denials?
If the organisation does not properly sequence any COB between the primary and the secondary insurance and does not have an EOB letter from the primary, then the secondary claims will auto-deny.
How often should payer contracts be reviewed to prevent denials?
No less than one time per year, and at the renewal of the payer contract, when a new payer is added, or quarterly upon the new Medicare Physician Fee Schedule being released.